
Islamabad the capital of Pakistan, has special status being the Federal Capital and is in the lime light of the world because of geo-political situation of the region. Population of Islamabad is 2.2 million. It is among the beautiful cities of the World with greenery all over, parks, lakes and hills. The city’s foundation was laid in 1962. There are 14 urban slums.
With the appearance of Corona Virus epidemic in the world the virus has slowly creeped in Pakistan and Islamabad.
ISLAMABAD CAPITAL TERRITORY
Epidemiological report:
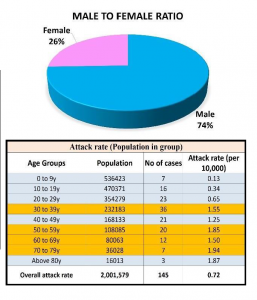
The national tally of confirmed COVID-19 cases in Pakistan has reached 6919. 145 positive cases, 17 recovered & 1 death have been confirmed in Islamabad so far.
MEASURES TAKEN BY MUNICIPALTY
The major interventions were at three levels
a) targeting screening of the travelers, b) hospital based interventions, c) community level surveillance and response.
Central Health Establishment under Ministry of Health (National Health Services Regulation and Coordination), has developed and implemented a screening program at the airports. The team at the air port ensure that the patient is fit to go home or needs to be investigated or need admission in the hospital.
At the hospital level the suspected patients are being screened and those positive are either admitted or advised quarantine at home, depending upon the condition.
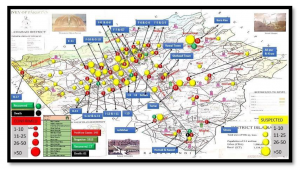
TRACING AND TRACKING THE CASE SURVELLENCE:
A) TRACING THE CASE
From 03 sources:
1.- From the Airport data
2.- From Hospitals
3.- From the community surveillance data
B) RISK ASSESSMENT
Risk is identified through
1.- Detailed history of the suspected patient on telephone.
2.- At the spot clinical history and examination by a doctor.
3.- Then categorizing patient and his contacts into
a) Suspected
b) Probable
c) Confirmed
C) TRACKING & CASE RESPONSE
a) Is being done by ⁿdesignated RRTs (Rapid Response Teams). RRTs are composed of:
– A Medical doctor
– A Medical technician
– A Driver
– A Security personal
b) After evaluation the decision is to be made whether;
i) the patient qualifies for the test of Corona Virus through NIH or not.
ii) is there a need to conduct tests for primary and secondary contacts or not.
iii) whether the patient need: – home quarantine – need referral and isolation / admission to hospital and – contacts need to he further investigated.
D) SOCIAL MOBILISATION
SM is done directly to the patient and his/ her contacts. Awareness creation is done and IEC material is distributed.
F) FOLLOWUP
is being Carried out by medical officers through telephone.
G) Daily report is generated and forwarded to the concerned
H) Data is analyzed regularly
I) Monitoring is through feedback mechanisms by random sampling methodology.
PROCESS AND STATISTICAL EVALUATIONS
1) Constitution of Rapid Response Teams (32 for DHO and 9 for MCI) in 3 shifts for case responses
2) Establishment of coordination offices by requisitioning services of admin officers and placing at disposal of DHS MCI for data basing and coordinating case responses
3) 6 Quarantine facilities established in collaboration with MoH.
4) Provision of doctors and staff along with equipment for upgrading the facilities/ services
5) Contacts of confirmed cases are shifted to Quarantine centers
6) Contact tracing of confirmed cases done by rapid response teams and home quarantine / isolation decided depending upon results from NIH. The same was adopted in G-13 and H-9 as well.
7) Around 190 returnees from KSA were all traced through phone calls and field visits by DHO field teams
8) Around 300 LHWs have delivered 12,086 lectures and distributed 10,000 brochures during tracing of suspected areas and house to house visits
9) Around 20,000 calls made to travelers of flights / people coming via land route (Iran)/ contacts of travelers and positive cases by ADHO ICT through data shared by NIH/FIA. The lists shared are being actively traced by field staff of DHS and DHO Office.
MOST SUCCESSFUL PRACTICES
1.- Coordinated effort between various departments
2.- A core team and central data collection and disbursement
3.- Support by District Administration]
4.- Support by Municipal Administration
4.- Political willingness.
5.- Intense media campaign
6.- Already existing Disaster Management Authorities.
BIGGEST CHALLENGES
1.- Initially lack of Coordination in the initial phase
2.- Dearth of PPEs and hospital based equipment i.e. ventilators
3.- Highly infectious viruses with totally new and unknown epidemiology and virulence
4.- Lack of available and trained human resource.
SUGGESTIONS TO OTHER CITIES
1.- Preventive measures should be initiated much before the intrusion of Corona Virus in the area / region/ country
2.- A very strong public health system including surveillance and response in the need of the hour in order to contain the infection at the community level.
3.- A through planning and strong coordination efforts.
MEASURES FOR ECNOMIC SUPPORT TO POOR
1. The industrial lockdown has badly affected the economic growth. However government has taken some measures to support the poor. These are:
a) Provision of food to the poor and in the lockdown areas
b) Provision of Rs.12000/- cash grant for hard ship because of current Covid 19 to each family under Ehsas program.
c) Tax exemption and services bill exemption / submission date extension.
![ISLAMABAD [MEASURES TAKEN BY MUNICIPALTY]](https://capitalsinitiative.com/wp-content/themes/rehub-theme/images/default/noimage_70_70.png)
